Physiologic hormones affecting the kidney
|
Hormone |
Trigger and pathway |
Site of action in the nephron (see figure) |
Net effect |
|
Angiotensin II (Ang II) |
Synthesized in response to hypotension. (See AKI and CKD chapters for details of Ang II production pathway) |
Afferent and efferent arteriole |
|
|
Atrial natriuretic peptide (ANP) |
Released in response to increased atrial pressure. |
Afferent and efferent arteriole, distal convoluted tubule (DCT). |
|
|
Vitamin D3 (calcitriol) |
Hypocalcemia |
DCT |
Increased calcium uptake. |
|
Parathyroid hormone (PTH) |
Hypocalcemia and hyperphosphatemia,and/or low vitamin D levels. |
Ascending limb of loop of Henle (LoH) and DCT |
Increased calcium uptake. |
|
Aldosterone |
Hypovolemia and hypotension (via Ang II), and/or hyperkalemia |
Collecting duct (CD) |
Increased sodium uptake and potassium excretion into the urine. Causes net fluid retention. |
|
Antidiuretic hormone (ADH) |
Hypovolemia and hypotension (via Ang II), increased plasma osmolality |
CD |
Increases free water uptake from the collecting duct. |
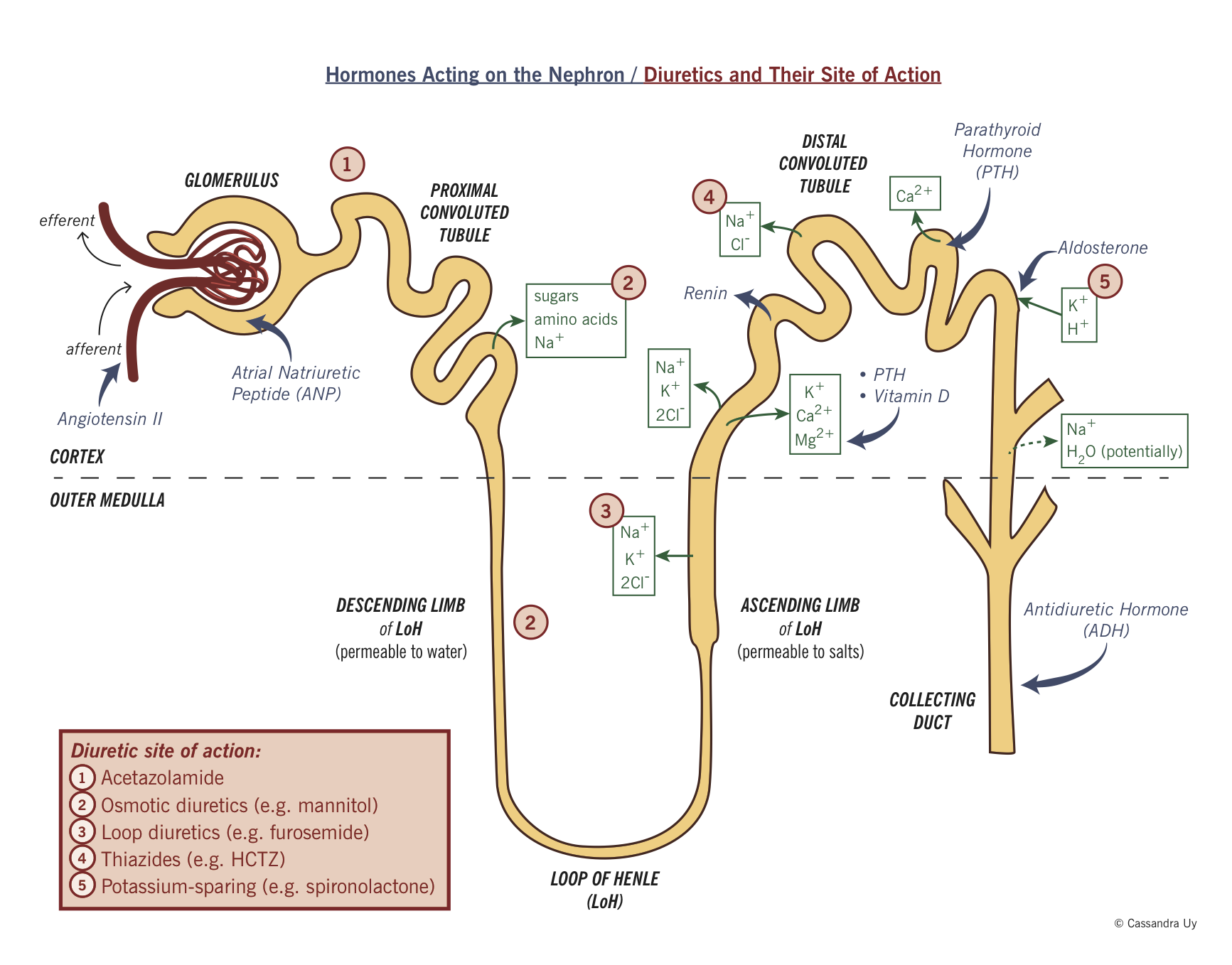
Diuretics
|
Diuretic type (example) |
Site of action |
Mechanism (see figure) |
|
Carbonic anhydrase inhibitor (acetazolamide) |
Proximal convoluted tubule (PCT) |
Acetazolamide is a carbonic anhydrase (CA) inhibitor. CA is an enzyme involved in the breakdown of carbonic acid in the following reaction: H2O + CO2 ←CA→ H2CO3 ↔ HCO3— + H+ Under physiologic conditions, filtered bicarbonate combines with the hydrogen ions to generate carbonic acid, which is acted on by CA to make CO2 and H2O. As the CO2 diffuses into the tubular cells, more bicarbonate is absorbed from the serum. In the presence of acetazolamide, CA is inhibited, allowing for the H2CO3 to build up in the tubules and hence urinary bicarbonate wasting (H+ alternatively is reabsorbed via a different pathway). This leads to a decreased ability to reabsorb Na+ in exchange for H+, leading to mild diuresis. |
|
Osmotic (mannitol) |
PCT |
Mannitol is filtered through the glomerulus but cannot be reabsorbed. This increases the osmolality of the filtrate and water is retained in the tubules to ensure urine osmolality. |
|
Loop (furosemide) |
Loop of Henle |
Blocks the sodium potassium chloride pump (NKCC) in the thick ascending limb of loop of Henle. This allows for more sodium and subsequently fluid loss from the nephrons. |
|
Thiazide (hydrochlorothiazide) |
DCT |
Thiazide diuretics block the activity of sodium chloride channels (Na-Cl) in the DCT allowing more sodium and water loss. |
|
Potassium Sparing
|
CD |
Aldosterone acts on the cells of the collecting ducts and induces expression of Na/K exchangers and ENaC. This allows for the exchange of sodium for potassium (Na enters the tubular cells and K is lost in the urine). Aldosterone antagonists competitively inhibit the action of aldosterone on the principal cells and therefore decrease the expression of the exchanger. With the lack of sodium uptake from the nephrons and loss in the urine, diuresis also takes place. Aldosterone also controls expression of ENaC channels in the distal tubules to absorb sodium. Inhibition of the ENaC decreases Na uptake and K loss from the tubular cells. Loss of Na in the urine leads to mild diuresis. |